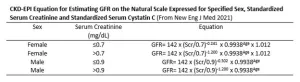
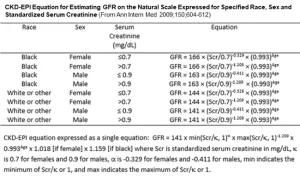
Creatinine measured in the blood is the most commonly measured endogenous filtration marker. It is a 113 Dalton amino acid derivative that is generated from the breakdown of creatinine in muscle, distributed throughout total body water, and excreted by the kidneys by glomerular filtration and tubular secretion. Although the blood level is affected primarily by the level of GFR, it is also affected by three other physiological processes (non-GFR determinants): generation by muscle mass and diet, tubular secretion by active transport, and extra-renal elimination by gastrointestinal or third space losses. Due to variation in these unmeasured processes, particularly creatinine generation, amongst individuals and within individuals over time, the normal value for creatinine differs among groups. The estimated GFR based on creatinine (eGFRcr) adjusted for demographic factors (age and sex) or clinical factors (weight and others) that are related to these processes, provides more information that the creatinine alone. All creatinine based estimating equations are limited by non-GFR determinants of creatinine that cannot be accounted for by the demographic and clinical factors. This is especially important in conditions associated with muscle wasting, as can be seen with severe acute or chronic illnesses. The Du Bois formula was used to calculate body surface area in the development of the CKD-EPI 2012 and 2021 equations.
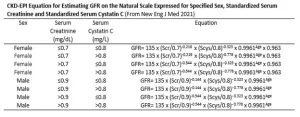
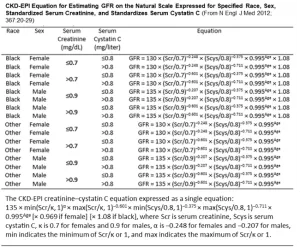
The 2024 KDIGO CKD guidelines recommended use of validated creatinine-based equations as the first step in GFR evaluation. As of 2025, the most commonly used equations are the 2021 CKD-EPI creatinine equation, and the 2021 European Kidney Function Consortium (EKFC) equation.